Objective Exam – Framework
This is the framework I use for my objective assessment. This is a work in progress…..so I don’t think that this is perfect and I certainly cannot ideally implement it exactly yet.
I am not going to talk about diagnostic/orthopaedic tests. They have their place in an exam, and certainly providing a specific structural diagnosis, when possible, is important. I am also not going to talk about physiotherapy specific testing that I/we might do. Rather I am going to talk about a clinical framework to classify the patients disorder, once we have diagnosed them.
My objective framework is, once again, based on this chart that I was exposed to when undertaking my postgraduate studies at the University of Western Australia.
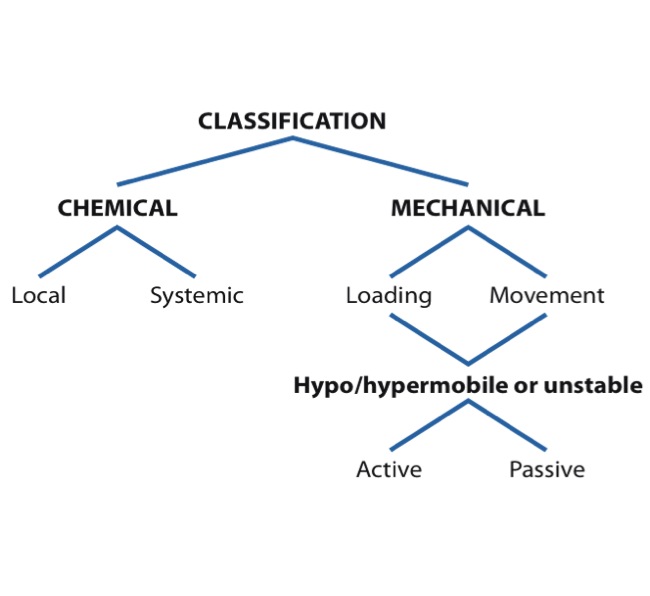
Prior to commencing on this classification process it is important that we have screened the patient for Red Flags and Pain Type (discussed previously). This will point us towards the patient have a mechanical (nociceptive) component that can be assessed in this framework. This framework can be used for inflammatory disorders, as is evident by the chemical side of the chart, but a large portion of our info in relation to this will be evident from our subjective. Neuropathic and Functional Pain cannot be assessed in this framework. Neuropathic pain can be assessed via Neuropathic screening tools (mentioned in a previous post). Functional pain can also be theorised following subjective exam and if no nociceptive, inflammatory or neuropathic basis for the pain can be concluded.
As mentioned earlier, one key step in the examination process is to reach a diagnosis. Whilst it is not always possible to identify a specific structure causing the pain, it is important that we do so if we can. I like to think of the diagnosis as the source of the patients symptoms. I then think of classification as identifying the cause of the patients problem i.e. what is causing the pain to occur i.e. is the cause a Loading/Control Impairment, a Movement Impairment, or a combination of both. Where I think physiotherapy goes wrong alot of the time is that a diagnosis is reached but then a very general, or recipe, based management process is implemented. I hope that following this post, and my subsequent case examples, that we will be able to see why a patient with, for example, a Flexion Movement Impairment at L5/S1 will need different treatment than a Flexion Control Impairment at L5/S1.
I base alot of what I do on Peter O’Sullivan’s framework for classifying Non-Specific Chronic Lower Back Pain (NSCLBP). My interpretation of this framework is that it is very similar to the diagram above. The following diagram from O’Sullivan, 2005, describes the interpretations of Movement Impairments vs Control Impairments in CNSLBP.

Whilst the above diagram refers to spinal pain in a number of areas, I do think that we can fairly easily apply these principles to peripheral joints as well.
Kangas et al (2011) utilise O’Sullivan’s framework in the classification of chronic foot pain. Some of the key points they make in regards to Control Impairments are:
- Lack of motor control drives the disorder.
- Patients pain is reproduced during functional tests and is related to an increased loading around the symptomatic area.
- Correcting the weight-bearing position and movement alignment of the foot and ankle often diminishes the pain immediately.
- During passive movement testing these is no movement restriction in the direction of pain.
In regards to Movement Impairments, Kangas et al (2011) describe to following key objective findings:
- Loss of normal physiological movement drives the pain disorder.
- The impaired movement direction becomes guarded, which contributes to an increase in stiffness.
- Attempts to correct the movement alignment (during the functional task) will result in increased impairment, protection and pain.
So hopefully we can now see the difference between a Control Impairment and Movement Impairment.
I think alot of the above can be difficult to explain without using case examples, hence my next post will begin this process.
References:
- O’Sullivan PB (2005) Diagnosis and classification of chronic low back pain disorders: maladaptive movement and motor control impairments as underlying mechanism. Manual Therapy. 10:242-255.
- Kangas J, Dankaerts W, Staes F (2011). New approach to the diagnosis and classification of chronic foot and ankle disorders: identifying motor control and movement impairments. Manual Therapy. 16:522-530.
About the Author: Mark Gibson
Mark is a Specialist Musculoskeletal Physiotherapist who consults at both Insight Physiotherapy and Pain Options, in Perth, Western Australia. He specialises in the assessment and management of persistent/chronic musculoskeletal pain. In addition to his clinical role he maintains regular involvement in education of the profession having held a Teaching Fellow position at the University of Western Australia for 10 years and regularly presenting at courses and seminars through the Australian Physiotherapy Association and private education sector. Mark is also a Facilitator for the Australian College of Physiotherapists Specialisation Training Program and a Sessional Academic at Curtin University. The views expressed on this blog are his own.Subscribe
If you enjoyed this article, subscribe to receive more just like it.




